Exploring the historical gaps in women’s hormone health and why more providers are approaching care with curiosity, listening, and personalized conversations.
Need to Knows
- Research, including preclinical models and clinical reviews, suggests that women’s hormone health influences systems beyond reproduction, such as sleep, mood, cognition, and cardiovascular health.1-3
- Hormone-related symptoms often overlap across conditions, life stages, and specialties, which can make them harder to recognize quickly or interpret in isolation.4
- Research gaps and male-centered clinical baselines have shaped how women’s hormone health has historically been studied, understood, and addressed.5
- As healthcare evolves, more providers are focusing on the 'whole person', prioritizing consistent, long-term care, truly listening to their patients, and having more tailored conversations about hormone health.
The Experience Many Women Share
For many women, the moment is familiar. Something in the body changes—persistent fatigue, brain fog, disrupted sleep, irregular cycles, hot flashes, mood shifts, or changes in energy and metabolism that do not quite make sense. During Women’s Health Month, these experiences offer an important reminder that women’s hormone health deserves thoughtful attention, not quick assumptions. When women bring these symptoms into a healthcare conversation, they are often looking for understanding and partnership in figuring out what may be happening.
Yet women’s hormone health has not always been approached in ways that make those experiences easy to interpret. Symptoms may appear gradually, overlap with other conditions, or affect multiple systems at once. They may not fit neatly into a single specialty or a single appointment.
As a result, some women leave healthcare conversations feeling that their concerns were minimized, normalized, or harder to explain than expected.6 Too many women have felt unseen or unsupported in their wellness journeys. At the same time, many providers are working within systems that were not designed for this level of nuance.
Why Hormone Symptoms Can Be Difficult to Diagnose
Hormone-related symptoms rarely appear in isolation. Because hormones influence many systems in the body,7 changes in hormonal signaling can present in many different ways, including:
- fatigue8
- sleep disruption9
- mood changes10
- brain fog11
- hot flashes or temperature changes12
- irregular menstrual cycles13
- low libido14
- acne, hair changes, or fluid retention15,16,17
- metabolic or weight-related shifts18
Many of these symptom patterns overlap with other conditions and life transitions. Stress, nutrition, thyroid function, sleep quality, metabolic health, reproductive stage, and medication use can all influence how symptoms appear.19
From patient to patient, the picture can look entirely different. A patient may describe fatigue, mood changes, and cycle irregularity in the same conversation, while another may present with sleep disruption, low libido, or changes in exercise tolerance. These presentations rarely map to a single, clear diagnosis.
For providers, this reinforces the value of looking for patterns over time rather than relying on a single symptom snapshot. Menstrual history, symptom timing, life stage, lifestyle factors, and broader clinical context often matter as much as any one data point.20
Patient communication also plays a central role. Open-ended questions, symptom tracking, and curiosity around timing and progression can help uncover patterns that might otherwise go unrecognized.

Research Gaps in Women’s Hormone Health
Women’s hormone symptoms have often been difficult to interpret in part because the research gap was not accidental. For many years, it was shaped by scientific assumptions, regulatory decisions, and the practical realities of study design.21
One of the most common scientific justifications for excluding women from research was the belief that hormonal fluctuations introduced too much variability.20 Compared with the relatively stable hormonal patterns observed in men, cyclical changes in estrogen and progesterone were often treated as confounding variables rather than as essential physiology worth studying.
From a study-design perspective, accounting for hormonal variability required more complex protocols. Researchers would need to consider menstrual phase, ovulation timing, and repeated measurements to understand how a woman responded to a medication, intervention, or stressor across the cycle. Rather than building that complexity into research design, many studies historically treated male physiology as the default baseline.22
Regulatory decisions also contributed to the gap. In response to serious historical drug-safety concerns, women of childbearing potential were restricted from participation in many early-stage clinical trials for years.23 Although those policies were intended to reduce risk, they also contributed to long stretches of limited data on how therapies and interventions affected women’s bodies.
Even when inclusion improved, practical barriers remained. Studying women’s hormone health often requires:
- larger and more diverse study populations
- cycle-specific testing and timing
- repeated laboratory measurements to confirm hormone status
- additional logistical coordination across variable biological rhythms
Those factors can make studies more expensive and time-intensive, influencing both design and funding decisions.
The effects of this gap are still visible today. In areas such as exercise physiology, metabolism, and even symptom interpretation, many established norms were built using male-centered data.24
As a result, some guidelines and expectations may not fully reflect how women experience physiological responses and treatment effects.25
For clinicians, this context helps explain why some patient experiences do not always fit neatly within traditional frameworks. In many ways, recognizing these gaps is part of a broader shift in healthcare—one that moves away from dismissal and toward deeper listening, better understanding, and more complete representation of women’s experiences.
Why Women’s Hormone Health Has Been Overlooked
Research gaps are only part of the story. Women’s hormone health has also been overlooked because healthcare has often approached it through a narrow lens.
For decades, hormone conversations were disproportionately centered on fertility, pregnancy, and menstrual regularity. But hormones also influence sleep, mood, energy, cognition, cardiovascular health, body composition, and how women feel in daily life.9,10,11,18
At the same time, healthcare is often divided by specialty. A woman might discuss cycle changes with one provider, fatigue with another, mood changes with another, and metabolic concerns somewhere else entirely. When symptoms are distributed across specialties, the underlying pattern can be harder to see.
There is also the issue of normalization. Symptoms that develop gradually are sometimes interpreted as stress, aging, burnout, or simply “what happens” at certain life stages. Sometimes that is part of the picture. Sometimes it is not. But when common symptoms are too quickly attributed to a broad explanation, women may feel important parts of their experience are being overlooked.
That is why this conversation matters. Women’s health deserves a better baseline—one that recognizes nuance instead of oversimplifying it.
The Shift Happening in Women’s Hormone Care
Across healthcare, the conversation around women’s hormone health is shifting, with more providers, researchers, and organizations recognizing that it deserves broader attention and more thoughtful care models.26 Rather than viewing hormone-related concerns as isolated symptoms, many clinicians are approaching them as part of a dynamic, interconnected system shaped by life stage, physiology, environment, and individual experience.
There is also growing awareness around conditions and transitions that have historically been under-discussed or under-recognized, including menopause, perimenopause, polycystic ovary syndrome (PCOS), endometriosis, and hormone-related metabolic changes. That awareness is helping create space for more informed, more nuanced conversations.
Better care begins with better questions—looking more carefully at patterns and recognizing that two patients with similar symptoms may not share the same underlying drivers or goals.
Clinical Reference: Key Hormones in Women’s Health, Common Symptom Patterns, and Provider Considerations
For provider readers, a quick-reference view can help anchor the broader discussion in a day-to-day clinical context.
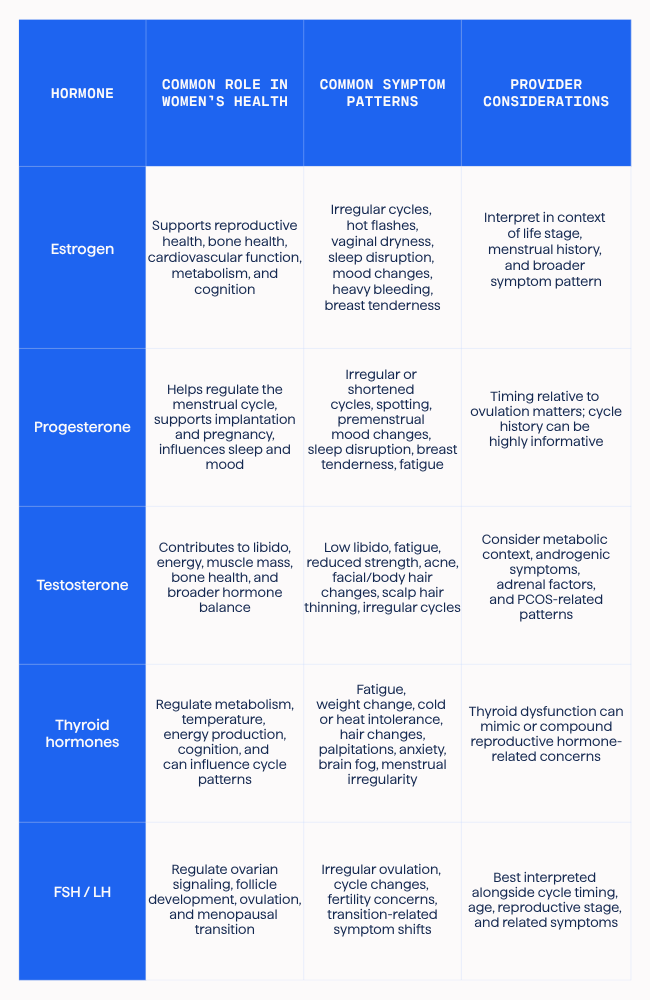
Hormone patterns rarely belong to only one symptom category, one life stage, or one specialty.
The Strive Approach to Hormone Conversations
At Strive, we anchor hormone conversations in three practical habits: listen early, look for patterns over time, and evaluate symptoms in a whole-person context.
Listen first
Patients often notice subtle changes before a clear clinical pattern emerges. Creating space for women to describe what feels different—in sleep, mood, cycles, energy, cognition, libido, or metabolism—can provide clinically useful context.
Look for patterns over time
Hormone activity is dynamic. Symptoms may change across menstrual cycles, stress levels, reproductive transitions, or lifestyle changes. Longitudinal assessment, symptom tracking, and follow-up conversations can reveal patterns that a single visit may miss.
Explore the whole picture
Hormone concerns do not exist in a vacuum. Thyroid function, metabolic health, nutrition, stress, sleep quality, training load, medications, and life stage can all shape how symptoms appear. A whole-person lens often leads to more informed conversations.
Defying Dismissal: What Women Deserve From Healthcare
For many women, understanding hormone-related symptoms begins with a simple but powerful experience: feeling heard.
Women’s hormone health rarely follows a simple checklist. It changes across life stages and can affect many dimensions of well-being. Recognizing that broader context does not make care less practical—it makes it more thoughtful.
Across healthcare, many clinicians are already striving against the status quo. They are asking deeper questions, listening more closely, and resisting the urge to reduce complex symptoms to easy assumptions. That matters, because behind every chart is a full life—a person with her own history, priorities, goals, and lived experience.
At Strive, we believe women deserve providers who listen, care models that honor the whole picture, and conversations that do not settle for oversimplification. We are proud to partner with clinicians who are leading the way forward in women’s wellness through trust, education, and partnership.
Because when healthcare moves away from dismissal and toward deeper listening, women’s hormone health is no longer treated as a side conversation. It becomes what it should have been all along: a vital part of whole-person care.
Continue the Conversation: Advancing Women’s Hormone Care in Practice
As the conversation around women’s hormone health continues to evolve, many providers are looking for ways to deepen their understanding and bring more clarity to clinical decision-making.
As part of this ongoing work, Strive Sessions is hosting a live webinar, Transform Your Clinical Approach to Women’s Health, focused on women’s health and bioidentical hormone therapy (BHRT). This session will explore how hormonal changes during peri- and post-menopause can shape patient experience, along with practical considerations around care approaches, patient selection, and clinical conversations.
Whether you’re already working in women’s health or beginning to expand into this area, this webinar is designed to support more informed, nuanced care—with space for live Q&A alongside Strive experts.
👉Click here to register for Transform Your Clinical Approach to Women’s Health.

References
- Ruehr L, Hoffmann K, May E, Münch ML, Schlögl H, Sacher J. Estrogens and human brain networks: a systematic review of structural and functional neuroimaging studies. Front Neuroendocrinol. 2025;77:101174. doi:10.1016/j.yfrne.2024.101174
- Daniel JM, Lindsey SH, Mostany R, Schrader LA, Zsombok A. Cardiometabolic health, menopausal estrogen therapy and the brain: how effects of estrogens diverge in healthy and unhealthy preclinical models of aging. Front Neuroendocrinol. 2023;70:101068. doi:10.1016/j.yfrne.2023.101068
- Baker FC. It’s not just about the hot flashes: menopausal hormone changes and disrupted sleep. J Clin Endocrinol Metab. 2023;108(2):e25-e26. doi:10.1210/clinem/dgac628.
- Mintziori G, Veneti S, Poppe K, et al. EMAS position statement: thyroid disease and menopause. Maturitas. 2024;185:107991. doi:10.1016/j.maturitas.2024.107991
- Zucker I, Prendergast BJ, Beery AK. Pervasive neglect of sex differences in biomedical research. Cold Spring Harb Perspect Biol. 2022;14(4):a039156. doi:10.1101/cshperspect.a039156
- Merone L, Tsey K, Russell D, Nagle C. “I just want to feel safe going to a doctor”: experiences of female patients with chronic conditions in Australia. Womens Health Rep (New Rochelle). 2022;3(1):1016-1028. doi:10.1089/whr.2022.0052
- Hiller-Sturmhöfel S, Bartke A. The endocrine system: an overview. Alcohol Health Res World. 1998;22(3):153-164.
- Zhang YD, Wang LN. Research progress in the treatment of chronic fatigue syndrome through interventions targeting the hypothalamus-pituitary-adrenal axis. Front Endocrinol (Lausanne). 2024;15:1373748. doi:10.3389/fendo.2024.1373748
- Buckley TM, Schatzberg AF. On the interactions of the hypothalamic-pituitary-adrenal (HPA) axis and sleep: normal HPA axis activity and circadian rhythm, exemplary sleep disorders. J Clin Endocrinol Metab. 2005;90(5):3106-3114.
- Lei AA, Phang VWX, Lee YZ, Kow ASF, Tham CL, Ho Y-C, Lee MT. Chronic Stress-Associated Depressive Disorders: The Impact of HPA Axis Dysregulation and Neuroinflammation on the Hippocampus—A Mini Review. International Journal of Molecular Sciences. 2025; 26(7):2940.
- De Alcubierre D, Ferrari D, Mauro G, et al. Glucocorticoids and cognitive function: a walkthrough in endogenous and exogenous alterations. J Endocrinol Invest. 2023;46(10):1961-1982. doi:10.1007/s40618-023-02091-7
- Zhang Z, DiVittorio JR, Joseph AM, Correa SM. The effects of estrogens on neural circuits that control temperature. Endocrinology. 2021;162(8):bqab087.
- Shao S, Zhao H, Lu Z, Lei X, Zhang Y. Circadian rhythms within the female hypothalamic-pituitary-gonadal axis: from physiology to etiology. Endocrinology. 2021;162(8):bqab117.
- Davis SR, Baber R, Panay N, Bitzer J, Perez SC, Islam RM, Kaunitz AM, Kingsberg SA, Lambrinoudaki I, Liu J, Parish SJ, Pinkerton J, Rymer J, Simon JA, Vignozzi L, Wierman ME. Global consensus position statement on the use of testosterone therapy for women. J Clin Endocrinol Metab. 2019;104(10):4660-4666. doi:10.1210/jc.2019-01603
- Carmina E, Dreno B, Lucky WA, Agak WG, Dokras A, Kim JJ, Lobo RA, Ramezani Tehrani F, Dumesic D. Female adult acne and androgen excess: a report from the Multidisciplinary Androgen Excess and PCOS Committee. J Endocr Soc. 2022;6(3):bvac003.
- Bienenfeld A, Azarchi S, Lo Sicco K, Marchbein S, Shapiro J, Nagler AR. Androgens in women: androgen-mediated skin disease and patient evaluation. J Am Acad Dermatol. 2019;80(6):1497-1506. doi:10.1016/j.jaad.2018.08.062
- Tsilosani A, Gao C, Zhang W. Aldosterone-regulated sodium transport and blood pressure. Front Physiol. 2022;13:770375. doi:10.3389/fphys.2022.770375
- Tao Z, Cheng Z. Hormonal regulation of metabolism—recent lessons learned from insulin and estrogen. Clin Sci (Lond). 2023;137(6):415-434. doi:10.1042/CS20210519
- Rigutto J, Steele C, Agrela AP, Brady G, Ester N, Papoutsa Shue A, et al. Thyroid, nutrition and lifestyle medicine: a feature review. Nutr Evid Database (NED), Br Assoc Nutr Lifestyle Med. Published March 2025. Accessed March 20, 2026.
- Rosen Vollmar AK, Mahalingaiah S, Jukic AM. The menstrual cycle as a vital sign: a comprehensive review. F S Rev. 2025;6(1):100081. doi:10.1016/j.xfnr.2024.100081
- Whelan AM. Unequal representation: women in clinical research. Cornell Law Review. 2021;106(4):1197-1248.
- Schmalenberger KM, Tauseef HA, Barone JC, et al. How to study the menstrual cycle: Practical tools and recommendations. Psychoneuroendocrinology. 2021;123:104895. doi:10.1016/j.psyneuen.2020.104895
- National Institutes of Health, Office of Research on Women’s Health. History of Women’s Participation in Clinical Research. Updated April 24, 2024.
- Elliott-Sale KJ, Minahan CL, de Jonge XAKJ, et al. Sex and gender in sports nutrition research: bridging the gap. Proc Nutr Soc. 2021;80(2):200-210. doi:10.1017/S0029665120006955
- Gualtierotti R. Bridging the gap: time to integrate sex and gender differences into research and clinical practice for improved health outcomes. Eur J Intern Med. 2025;134:9-16. doi:10.1016/j.ejim.2025.01.030
- Williams JS, Fattori MR, Honeyborne IR, Ritz SA. Considering hormones as sex- and gender-related factors in biomedical research: challenging false dichotomies and embracing complexity. Horm Behav. 2023;156:105442. doi:10.1016/j.yhbeh.2023.105442